


Every workforce has an MSK problem. Back pain, neck pain, joint injuries, and repetitive stress conditions affect workers across every industry and every kind of role. But the similarity ends there.
The way MSK conditions develop, where they show up, how severe they become, and what gets in the way of care all vary significantly depending on how someone spends their workday. The desk worker who has been sitting in a poorly set-up home office for three years develops pain differently than the warehouse employee lifting repetitively on a twelve-hour shift, or the electrician navigating a new job site every week. Their risk patterns are different. Their barriers to getting help are different. And the care that works for each of them is different.
Yet most employer MSK benefits are designed as if those differences don’t exist. A single program, built around a single modality, applied uniformly across a population that is anything but uniform. The result is predictable: some workers are well served, and the rest quietly go without.
The HR leaders who are seeing the best outcomes, lower claims, higher adherence, fewer surgeries, aren’t necessarily spending more. They’re asking a more precise question: what does work actually look like for our people, and does our MSK strategy account for that?
MSK Is Universal. The Risk Profile Isn’t.
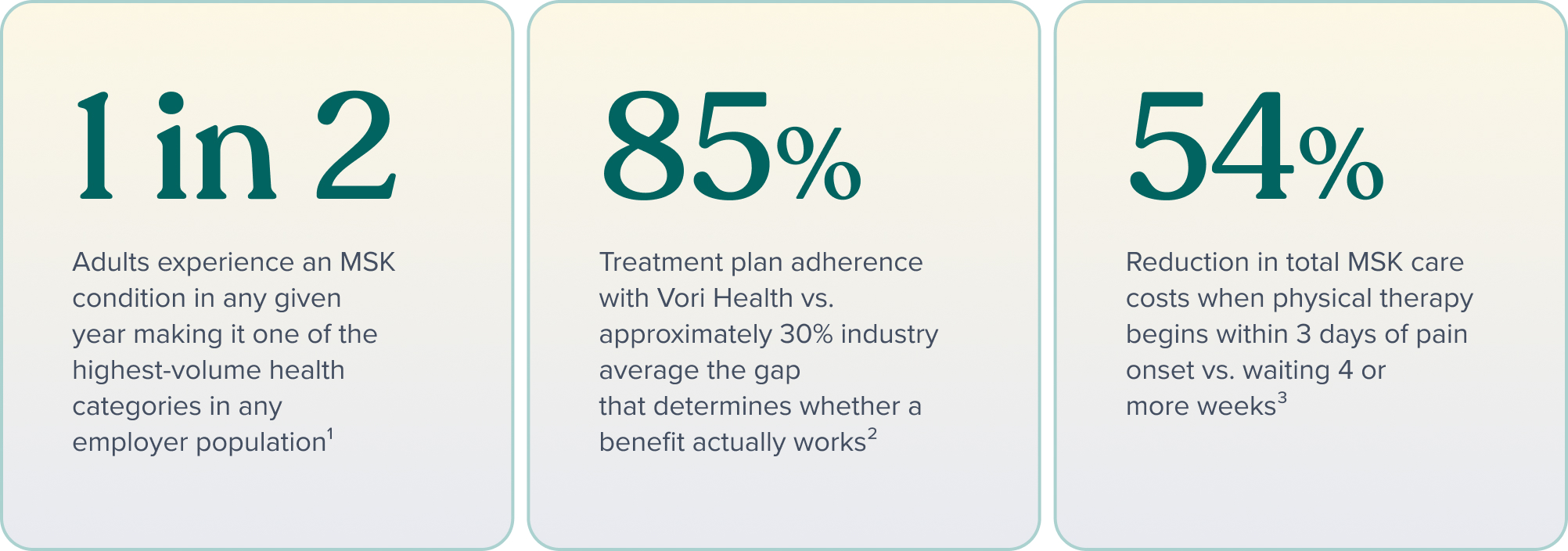
One in two adults experience an MSK condition in any given year.¹ Across the full working population, that makes MSK one of the highest-volume health categories any employer is managing, and one of the most expensive when care is fragmented or delayed.
What the aggregate number doesn’t capture is how differently MSK risk manifests depending on the nature of the work. For most benefits leaders, MSK strategy defaults to whichever population is largest or most visible, often desk workers, because they’re the majority in many organizations. That leaves physical and field-based workers with a benefits design that wasn’t built for them, and the consequences accumulate quietly in claims data and workforce availability.
Understanding the distinct risk patterns across workforce types isn’t just an academic exercise. It’s the foundation of any MSK strategy that actually performs.
Three Workforce Types, Three Different Problems
DESK AND REMOTE WORKERS: THE SLOW ACCUMULATION RISK
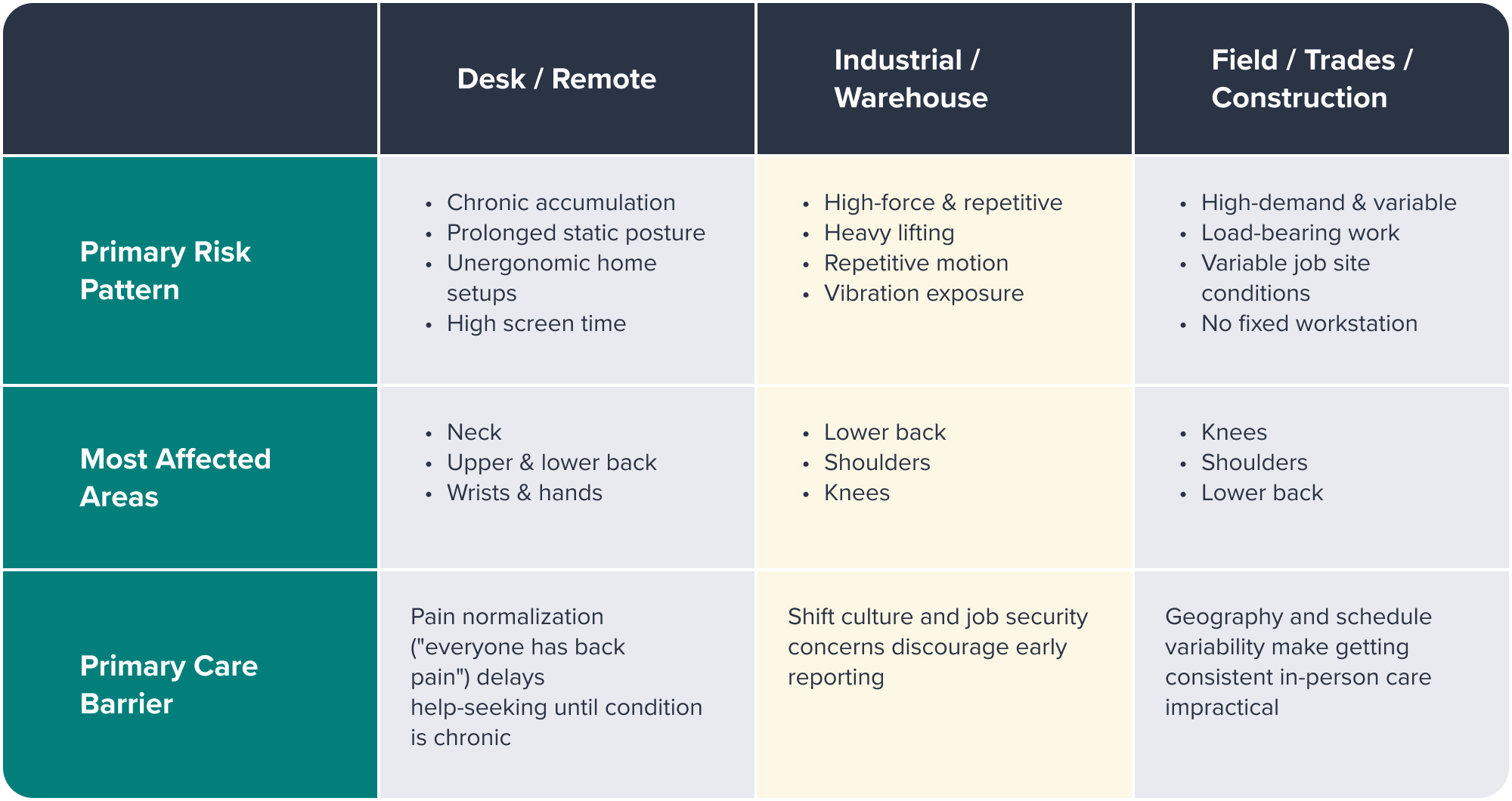
The risk for desk and remote workers is chronic rather than acute, it builds gradually through prolonged static posture, extended screen time, and the kind of minimal movement that modern knowledge work demands. In any given year, between 42% and 69% of sedentary office workers experience neck pain, and between 31% and 51% experience lower back pain.6 Neck pain is now more prevalent among office workers than in any other occupation.
The shift to remote and hybrid work added a new layer of risk that benefits strategies largely haven’t caught up with. When employees moved home, they brought their workloads but left their ergonomic infrastructure behind. Dining tables, couches, and kitchen stools became workstations. Research shows that remote workers with poor home setups have more than twice the odds of developing new neck or upper back pain compared to employees in properly equipped office settings.7
The care barrier here is cultural as much as logistical. Desk workers are more likely than other workforce types to normalize early pain, to accept back pain and neck stiffness as an inevitable byproduct of the job. That normalization delays help-seeking until an acute, manageable condition has become chronic. By the time the claim appears, the window for low-cost, conservative intervention has often closed.
INDUSTRIAL, MANUFACTURING, AND WAREHOUSE WORKERS: THE HIGH-FORCE, REPETITIVE RISK
For workers in industrial, manufacturing, and warehouse environments, the MSK risk profile is defined by physical demand: heavy lifting, repetitive motion, awkward postures sustained across long shifts, and vibration exposure from equipment. These are not sedentary conditions. The body is under consistent mechanical load, often without adequate recovery time built into the schedule.
The injury pattern reflects that. Lower back, shoulder, and knee conditions are most prevalent in these settings, and they tend to be more acute in onset than the gradual accumulation seen in desk workers. A single lift under load, a repetitive motion performed thousands of times, a sustained posture held for hours, any of these can be the visible trigger for a condition that’s been developing quietly.
The care barrier in industrial and warehouse environments is cultural and structural. Workplace norms in physical industries often treat pain as part of the job, something to push through rather than address. Reporting pain early can feel like a risk: a concern about being seen as unable to do the work, reassigned, or pulled from a shift. That silence comes at a cost. Conditions that would have resolved with early conservative care escalate into the kinds of injuries that drive workers’ compensation claims and long-term disability.
Access is also a practical constraint. Shift schedules, irregular hours, and facilities located away from urban centers can make standard daytime appointment models effectively inaccessible. A benefits strategy that doesn’t account for that isn’t really available to this population, regardless of what it says on paper.
FIELD-BASED, TRADES, AND CONSTRUCTION WORKERS: THE HIGH-DEMAND, VARIABLE RISK
Field-based workers, in construction, trades, utilities, and similar industries, face the most physically variable MSK risk environment of the three. Unlike industrial workers who perform consistent tasks in a fixed facility, field workers navigate different physical demands across different job sites, often week to week. Load-bearing work, overhead and kneeling postures, equipment operation, and exposure to uneven terrain create a diverse injury pattern with knees, shoulders, and lower back most commonly affected.
These workers are also among the most likely to be skeptical of traditional healthcare pathways. Many have had the experience of being told to rest and take pain medication, or of being steered toward surgery before conservative options were fully explored. That history shapes how they engage, or don’t engage, with benefits designed for a different kind of care experience.
The access barrier for field workers is geographic and logistical. A worker who is at a different job site every week cannot reliably attend appointments at a fixed clinic. A benefits design that requires in-person visits at a specific location effectively excludes this population. Virtual care, when it’s genuinely integrated rather than tacked on, changes that equation, making care available wherever the worker happens to be.
What a One-Size-Fits-All MSK Benefit Actually Costs
The appeal of a uniform MSK benefit is understandable. It’s administratively simpler, easier to communicate, and easier to evaluate in the aggregate. The problem is that aggregate performance masks population-level gaps.
When a benefits program achieves 30% treatment adherence, roughly the industry average, the reasons behind that number vary significantly by workforce type. The desk worker who doesn’t engage may not see the benefit as relevant to their “normal” back pain. The warehouse employee may not be able to access it given their shift schedule. The field worker may not trust a care model that doesn’t understand their occupational demands. The problem looks the same from the data, but the solution is different for each.
Low adherence isn’t just a communications problem, it’s usually a design problem. When the care model doesn’t fit the worker’s life, the worker doesn’t use it. The employer pays for a benefit that isn’t being used, and pays again for the downstream claims that result.
For mixed workforces, a single-modality solution, virtual-only or in-person-only, structurally excludes part of the population by design. That exclusion is invisible in the enrollment numbers and only becomes visible when claims data or workforce availability data surfaces the consequences.
The more precise question for any HR leader managing a mixed workforce isn’t “what is our MSK benefit?” It’s “what is our MSK benefit doing for each of our workforce populations, and what is it missing?”
What Personalized MSK Care Actually Looks Like
Personalization starts at the first visit, but it doesn’t stop there. Rather than routing members through a referral chain to disconnected providers, an effective MSK care model meets each member where they are with what they actually need.
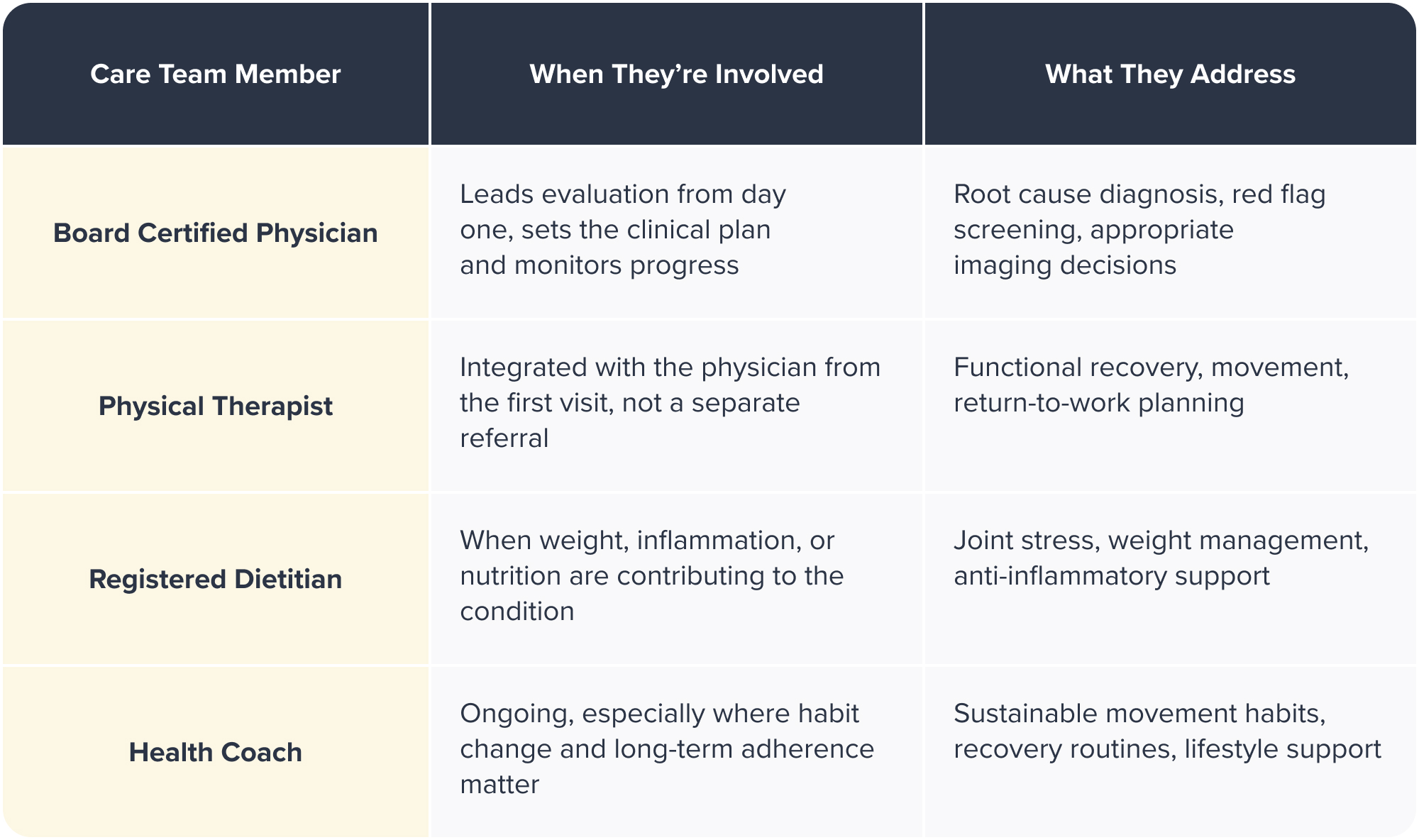
That might mean a board-certified physician and physical therapist working together on day one.
It might mean a registered dietitian supporting a warehouse worker managing weight-related joint stress alongside a repetitive motion injury.
It might mean a health coach helping a field employee build sustainable movement habits that hold up across variable job site conditions.
The team, physicians, physical therapists, registered dietitians, and health coaches, works together in-house, coordinating in real time rather than communicating across separate systems and separate schedules.
For HR leaders managing mixed workforces, this matters because the right intervention looks different depending on the worker. A desk employee with chronic neck pain needs something different than a construction worker recovering from a shoulder injury or a warehouse employee managing knee pain from years of repetitive motion. A care model built around a single modality will serve some of those people well and the rest poorly. A fully integrated team can meet all of them.
The structural advantage that makes this work is having everyone in-house. No delayed referrals, no disconnected handoffs, no member left trying to coordinate care between providers who don’t talk to each other. The care team already knows the full picture before the member’s next interaction, and the plan adjusts accordingly.
The other dimension of personalization is modality. A benefits strategy that only works for workers who can attend daytime in-person appointments is not a strategy for most industrial or field workers. Genuine hybrid care, where virtual and in-person access are both first-class options, not a primary model with a workaround attached, is what makes an MSK benefit genuinely available across a mixed population.
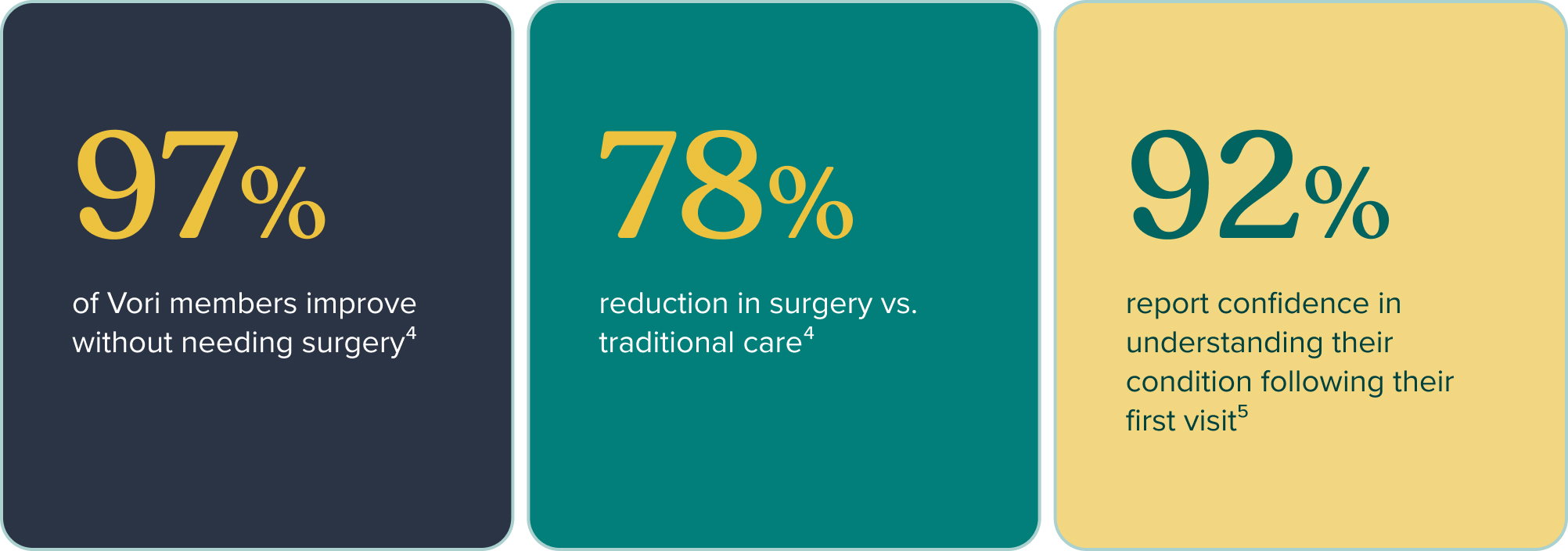
These outcomes are not population-specific, they reflect what happens when care is designed to meet the member rather than asking the member to navigate the system. The 85% adherence figure is the most telling: it’s the result of a model where workers across workforce types find the care accessible, credible, and relevant to their situation.
Three Questions to Audit Your Current MSK Strategy
1. Does our MSK benefit work equally well for every type of worker in our population?
Most benefits leaders can answer this question for their largest or most visible workforce segment. Fewer can answer it for every segment. If the answer is “I’m not sure,” that uncertainty is worth investigating before the next claims cycle makes it clear.
2. What does our treatment adherence data look like, and can we see it by workforce type?
A plan-level adherence number of 30% looks the same whether the benefit is underperforming uniformly or whether it’s working well for some populations and failing others entirely. Segmented adherence data tells a more useful story.
3. When a warehouse employee or field worker needs MSK care, what does their actual journey look like?
Walk through the steps. How do they access the benefit? Does the scheduling work for their shift? Is there a virtual option that doesn’t require them to take time off? Is the clinical team familiar with their kind of work? The friction in that journey is where a well-intentioned benefit loses the people it’s supposed to serve.
The Case for Building It Right
The employers who are getting ahead of MSK costs aren’t necessarily spending more. They’re spending more precisely on care that actually fits the people using it.
For mixed workforces, that means moving past the search for a single MSK solution and toward a strategy that accounts for distinct risk profiles, distinct care barriers, and distinct access needs. It means an integrated care team that can meet the sedentary worker, the shift worker, and the field worker with something relevant to each of them. And it means a benefits design where adherence is high not because the program is well marketed, but because it actually works for the people enrolled in it.
When MSK care is built around the workforce rather than applied uniformly to it, the outcomes, for people and for the organization, follow.
Tell us about your workforce. We’ll show you how Vori’s care team maps to your population mix: desk workers, industrial employees, and field teams included—request a benefits demo today.
CITATIONS
1. Business Group on Health / U.S. Bone and Joint Initiative (2023). 1 in 2 adults experience an MSK condition annually. businessgrouphealth.org
2. Vori Health / Validation Institute (2023). 85% treatment plan adherence vs. ~30% industry average; 97% of members improve without surgery; 78% reduction in surgery vs. traditional care. vorihealth.com/resource/new-validation-institute-report-affirms-vori-health-care-model
3. Sword Health, citing published research. Starting PT within 3 days of low back pain onset reduces total cost of care by up to 54% vs. waiting 4+ weeks. swordhealth.com/articles/reduce-employer-healthcare-expenses
4. Vori Health / Validation Institute (2023). See citation 2.
5. JMIR Formative Research (2025). 92% of Vori Health members report increased confidence in understanding their condition and treatment plan after their first integrated visit. vorihealth.com/resource/vori-health-cuts-care-delays-boosts-treatment-confidence
6. PMC / Pain Reports (2022). One-year prevalence of neck pain ranges from 42–69% and lower back pain 31–51% among sedentary office workers. pmc.ncbi.nlm.nih.gov/articles/PMC9128793
7. PMC (2025). Remote workers with poor workstation setups had more than twice the odds of new neck or upper back pain (OR 2.02, 95% CI 1.08–3.76) vs. office-only workers. pmc.ncbi.nlm.nih.gov/articles/PMC12039904
8. Cagnie B et al. (2007), European Spine Journal. 56.2% of office workers with neck pain reported their complaints started during their current job. pmc.ncbi.nlm.nih.gov/articles/PMC2213555
© 2026 Vori Health.
For informational purposes only. Does not constitute medical or financial advice.


